

Pans and Pandas
Sudden changes of mental health in children may be because of PANS/PANDAS.

The Chicago suburbs are a diverse and bustling outstretch of the urban center of Chicago. They are mixture of middle and upper-class neighborhoods, private and public schools, parks and playgrounds and provide a wide access of public and private services. Residents have access to top schools, top doctors, and a wide array of professional services. It’s everyday America.
Daniel, a 7-year-old, living his both his parents and 2 other siblings in the Chicago suburbs had always been an easy-going, active kid, and mostly had a healthy early childhood. Almost like a light switch turned off, he changed. Literally it seemed to his parents Sarah and Michael that it was overnight. He started getting anxious about everything. The way he looked in the mirror, the texture of the food, the way he washed his hands, the time his parents were going to pick him up for school, and so on and so on. Nothing seemed to be off limits for his anxiety and worry. In addition, they started notice a motor tic; where he would blink his eyes receptively for no reason.
Teasing happened. Kids at school started asking him questions and he became angry and aggressive with them. His playdate calendar started to decline. They started avoiding him. It was very confusing and sad to Daniel and his family.
After setting up an appointment with their pediatrician there was some hope to get some answers. The pediatrician took a careful history and physical exam and suggested neuropsychiatry testing and suggested that Daniel might have obsessive compulsive disorder (OCD) and may need to go on medications.
Sarah and Michael were besides themselves. How could things change overnight? A medication? A serious psychological diagnosis? How? Why?
This worry consumed their late nights especially. Sarah would get on the computer after finally getting the kids to bed and was googling symptoms trying to find an answer. Of course, she would land on the worst of the worst conditions popping up in the search and so she would go down the rabbit hole of worry.
Sarah landed on something was called Pediatric Acute Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS). PANDAS is subset of Pediatric Acute Neuropsychiatric Syndrome (PANS). After, seeing that hallmark of PANDAS was sudden neuropsychiatric changes in a child days to weeks after having a streptococcal infection; she felt a wave of relief. Sarah remembered that Daniel had Strep throat about 10 days before all of these symptoms started. At the time they started at urgent care for penicillin and he seemingly felt better. Yet, these neuropsychiatric symptoms started 10 days later. Since she found this connection; she again reached out to the pediatrician.
Her pediatrician listened but still felt strongly that Daniel should see the neuropsychiatrist and asked Sarah to stick with the plan. This didn't sit well with Sarah and she began looking for specialists in PANDA's. Finally, after a search on pandasnetwork.org she found a provider who specialized in PANDAS and scheduled an appointment.
The Diagnosis of PANS/PANDAS is a diagnosis of exclusion when other concerns have been ruled out including Autoimmune Encephalitis, CNS vasculitis, neuropsychiatric systemic lupus erythematosus (NPSLE), acute disseminated encephalomyelitis (ADEM), and Bechet’s disease. (Frankovich et al., 2017)
PANS /PANDAS is defined by the foudroyant (lightning-like) onset of obsessive– compulsive disorder (OCD) or eating restrictions and comorbid symptoms from at least two of seven categories: anxiety (particularly separation anxiety); emotional lability or depression; irritability, aggression, and/or severely oppositional behaviors. It has been estimated that OCD may begin as early as 1–3 days before the onset of Group A-Streptococcal (GAS)-pharyngeal symptoms (i.e. Sore throat), and as late as 30 days or more after the GAS infection. (Thienemann et al., 2017)
In addition, PANS and PANDAS suffer from tics (about 70%), ADHD, sensory or motor abnormalities (dysgraphia), sleep disturbances, enuresis, and urinary frequency.(Frankovich et al., 2017; Thienemann et al., 2017)
The tics can be particularly troubling. Some may be more complex motor of vocal tics that may even present like Tourette syndrome.
Oppositional, rage, or anger episodes often last 45-60 minutes and upon calming down the child often doesn't even know they behaved the way they did and feel remorseful.
In some kids they will experience mitochondrial dysfunction. Mitochondria being the cells that produce energy in the body including the brain. Mitochondrial dysfunction can be with symptoms of hypotonia (weak pencil grasp, low core strength, difficulty pumping swing, sitting in the W-position). In addition, mitochondrial regression can present with multiple regressions, low energy, easy fatigue, clumsiness, constipation, and speech /articulation issues.(Song, 2018)
Group A strep in the cases of PANDAS becomes an issue when it evades and impairs host defenses. In that it can avoid phagocytic engagement, inhibit complement and antibody functions required for opsonization, it can inhibit compliment and antibody functions required for opsonization, it can impair phagocytic uptake mechanism, and resist phagocytic killing mechanisms (like antimicrobial peptides and reactive oxidative species).(Crista, 2023; Song, 2018) . The autoimmune component of PANDAS is explained by molecular mimicry. The foreign antigen shares sequence similar to self-antigens.
In Pandas, components of the Group A strep cell walls cross react with the neurons in the basal ganglia caudate, putamen, and internal segment of the globus pallidus.
Further, anti-neuronal autoantibodies react with the brain including Lysoganglioside, dopamine receptors, activation of the calcium-calmodulin dependent protein kinase II (CAMKII), or tubulin. (DOP,2020)
In mice studies, autoantibodies that target the CMKII enzyme and target the Dopamine receptor (D2) will result in obsessive behaviors. Other pathways studied such as Lysoganglioside and tubulin are also seen in Sydenham's Chorea. (DOP, 2020)
There are appears to be wide spread neuro-immune inflammation in PANS/Pandas involving alterations of regulatory T-cells, immunoglobulins, cerebrospinal fluid, oligoclonal bands, and immune-associated genes. (DOP<2020). Up to 80% of PANS patients have immune abnormalities(Frankovich et al., 2017). There is evidence of TH17 antibody activity and responses including (interleukin-6 and trans- forming growth factor beta) and antibody production in PANS/PANDAS. This is the premise of the use of immunomodulatory therapies in PANS/PANDAS.
The history of the case will determine the basis for PANS and PANDAS testing. For example, abrupt neuropsychiatric behavior changes that followed a strep infection would lead more to a PANDAS approach to testing, however, abrupt neuropsychiatric behavior change not necessarily following strep would lead to more of a PANS approach. Still, the timing of diagnosis is usually very late and catching clues on a lab test is not often achieved.
The earlier the work up these conditions the better.
For example, for suspected PANDAS initial testing would include
1. Cultures of throat, nose, skin, and sometimes anus.
2. Anti-streptolysin antibodies (ASO) and ANTI-DNASE B strep antibody
3. Cunningham Panel: anti-dopamine D1 receptor, anti-dopamine D2L receptor, Anti-lysoganglioside-GM1, anti-tubulin. Antibodies against the D1 receptor may result in psychosis, ocd, and tics. Whereas antibodies against the D2L receptor, may result in impulsivity, uncontrolled movements, and hyperactivity. Lysoganglioside GM1 is located within the membrane of nerve cells and is highly concentrated in the central nervous system. It functions as insulation around the nerve cell and plays an important role in signal transmission in the brain. It provides a vital function in communication between neurons and ensures proper transmission of impulses. Individuals with elevated levels of anti-Lysoganglioside GM1 often reported having sleep disturbances, behavioral regression, and obsessions/compulsion. Tubulin is an intracellular protein that forms microtubules and provides a skeleton for maintaining cell shape and is thought to be involved in cell motility and intracellular transport. Tubulin is contained within most every cell and is highly abundant and concentrated in brain cells. It plays an important role in cell signaling and communication within the cell. When a patient’s autoantibodies are directed against Tubulin, OCD-like symptoms and cognitive impairment, such as ‘brain fog’ have been reported. The Calcium/calmodulin-dependent protein kinase II (CaMKII) is a key enzyme that is involved in the upregulation of neurotransmitters: dopamine, epinephrine and norepinephrine. CaMKII enzyme would be up-regulated in PANDAS. (“What Does The Cunningham Panel Measure? - Moleculera Labs,” 2024)
The Cunningham has poor specificity for PANDAS 10% and PAN 6%, and variable negative predictive values (44-74%); making it a relative longshot tool that should be used scrupulously. (Dop et al., 2020)
An investigation of PANS may look at broad factors including:
1. CBC often decreased WBC
2. Total IgG with subclasses IgA, IGM
3. ANA with reflex
4. Celiac Panel
5. Lyme and Co-infections (Borrelia burgdorferi, Babesia, Erlichia, Bartonella, Rickettsia)
6. Epstein Barr Virus
7. Mycoplasma pneumonia
8. HSV 1&2,
9. Coxsackie Virus A+B,
10. parvovirus B-19, IgG
11. Cytomegalovirus (CMV) IgG
12. influenza
13. Candida
14. SARS-CoV-2-
15. Heavy Metal Toxicity
16. Mycotoxin and Mold
The investigation of Mitochondrial function can be seen on lab testing including Organic Acid testing.
Abnormal mitochondrial function may show as:
1. elevated ast, alt
2. elevated creatine kinase
3. elevated lactate (performed stat)
4. elevated pyruvate (performed Stat)
5. Elevated fasting ammonia (performed fasting and stat)
6. Decreased free and total carnitine
7. Abnormal acylcarnitine profile
8. Decreased or suboptimal Co Q10
9. Fasting plasma organic acids high in alanine or Alanine: Lysine >3
10. Mito swab testing can also be performed.
However, while these tests may provide confidence and confirmation; here is some uncomfortable truths about PANS/PANDAS that child/family is often faced with:
1. PANS/PANDAS is often a clinical diagnosis
2. The child and family won't know if the diagnosis is right until they start treating,
3. Chances are that many psych meds will be prescribed and tried before actually getting a diagnosis.
4. PANS and PANDAS is not widely accepted and is considered controversial by some of the medical community
5. Patients don't recover from PANS/PANDAS by just taking an antibiotic. While important it takes much more treatment and therapies then taking an antibiotic
6. The hallmark of PANS/PANS is the abrupt onset of neuropsychiatric symptoms rather than lifelong progression of certain neuropsychiatric symptoms.
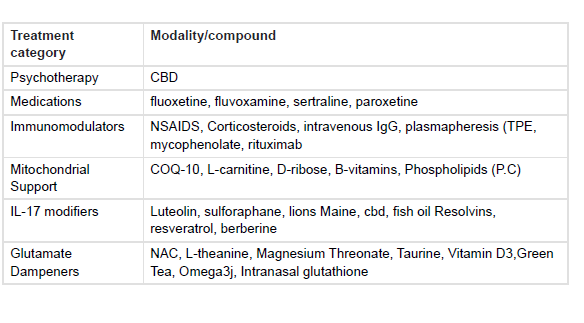
Many times, the clinician will start with treatment with strategies to stabilize symptoms especially OCD. Calm inflammation, and address infectious components. As mentioned there is neuroimmune inflammation taking place in PANS/PANDAS and conventional medications (i.e., steroids, IVIG) and other immunomodulators (plasmapheresis) are sometimes used. There are many natural supplements (see chart) that dampen TH17 activation and glutamate excess that can also be employed. Most if not all children will need counseling and possibly medication to help with anxiety, ocd, and/or depression. Specific symptomatic treatments can be provided for tics. Since mitochondrial dysfunction is common; such a dysgraphia; there may be need for mitochondrial nutrients.
I recently had a podcast with Nancy O'hara, MD . Dr. O’hara is an expert in this topic and author of Demystifying PANS/PANDAS: A Functional Medicine Desktop Reference on Basal Ganglia Encephalitis,
In the episode we covered:
Dr. O'Hara's approach and Philosophy work.
The life and tribulations of a family with a medically challenged child.
3-pronged approach (Treat symptoms, treat inflammation, treat-infection)
Making a diagnosis. The challenges of testing and the importance of the clinical diagnosis.
How Sars-Cov-2 spike protein has impacted PANS/PANDAS due to its impact on latent viruses and vector borne illness.
More About Dr. O'Hara
Dr. Nancy O’Hara is a board certified Pediatrician. Prior to her medical career, Dr. O’Hara taught children with autism. She graduated with highest honors from Bryn Mawr College and as a member of the Alpha Omega Alpha Honor Society from the University of Pennsylvania School of Medicine. She earned a Master’s degree in Public Health from the University of Pittsburgh. After residency, chief residency and general pediatric fellowship at the University of Pittsburgh, Dr. O’ Hara entered general private practice in 1993, and in 1998 began her consultative, integrative practice solely for children with special needs. Since 1999 she has dedicated her functional medicine practice to the integrative and holistic care of children with chronic illness and neurodevelopmental disorders such as ADHD, PANDAS/PANS, OCD, Lyme and ASD. She is also a leader in the training of clinicians, both in the United States and abroad. Dr. O’Hara has written a comprehensive guidebook, “Demystifying PANS / PANDAS: A Functional Medicine Desktop Reference on Basal Ganglia Encephalitis”, which is available on Amazon in e-book or soft-cover formats. For more information on her membership and mentoring program, please visit www.drohara.com. Additionally, Dr. O’Hara’s research on Folate Receptor Auto Antibodies and PANS/PANDAS was recently published. (https://doi.org/10.3390/jpm14020166)
Resources that were mentioned in the episode that may be helpful:
1. Spellers https://spellers.com/
2. Medical Academy of Special Needs: About Us - MAPS
3. Neurobiology of Everyday communication https://pubmed.ncbi.nlm.nih.gov/27284021/
4. Helminth Therapy Human helminth therapy to treat inflammatory disorders- where do we ...
5. Toxicant Load in Liver disease https://www.ifm.org/news-insights/addressing-body-burden-discussion-lyn-patrick-nd-toxicants/
7. Socio-medical studies of individuals self-treating with helminths ...
8. Hymenolepis diminuta Cysticercoids Production and Use of Hymenolepis diminuta Cysticercoids as Anti ...
9. Biome Restoration https://biomerestoration.com/
10. Demystifing Pans and Pandas book by Dr. O’Hara https://www.amazon.com/Demystifying-PANS-PANDAS-Functional-Encephalitis/dp/1939794269?ref_=ast_author_dp
11. Mentorship program by Dr. O’hara https://www.drohara.com/membership
You can listen to the podcast episode here :
Related episodes
Panda/Pans with Jill Crista, ND https://www.onethingpod.com/s5e84
The Immune System and Mental Health with Dr. Emily Gutierrez https://www.onethingpod.com/s6e93
Mitochondrial Dysfunction and Autism with Richard Bolles, MD
https://www.onethingpod.com/mitochondrial-dysfunction-and-autism-with-dr-richard-g-boles/
Please support our sponsors and affiliates:
https://www.onethingpod.com/sponsors/
References:
Crista, J. (2023). A light in the dark for PANDAS & PANS. Dr. Jill Crista.
Dop, D., Marcu, I., Padureanu, R., Niculescu, C., & Padureanu, V. (2020). Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (Review). Experimental and Therapeutic Medicine, 21(1), 94. https://doi.org/10.3892/etm.2020.9526
Frankovich, J., Swedo, S., Murphy, T., Dale, R. C., Agalliu, D., Williams, K., Daines, M., Hornig, M., Chugani, H., Sanger, T., Muscal, E., Pasternack, M., Cooperstock, M., Gans, H., Zhang, Y., Cunningham, M., Bernstein, G., Bromberg, R., Willett, T., … Thienemann, M. (2017). Clinical management of pediatric acute-onset neuropsychiatric syndrome: Part II—use of immunomodulatory therapies. Journal of Child and Adolescent Psychopharmacology, 27(7), 574–593. https://doi.org/10.1089/cap.2016.0148
Song, E. (2018, August 18). Brains On Fire. Integrative Medicine For Mental Health.
Thienemann, M., Murphy, T. K., Leckman, J. F., Shaw, R. J., Williams, K., Kapphahn, C. J., Frankovich, J., Geller, D., Bernstein, G. A., Chang, K., Elia, J., & Swedo, S. E. (2017). Clinical Management of Pediatric Acute-Onset Neuropsychiatric Syndrome: Part I—Psychiatric and Behavioral Interventions. Journal of Child and Adolescent Psychopharmacology, 27(7), 566–573. https://doi.org/10.1089/cap.2016.0145
What Does The Cunningham Panel Measure? - Moleculera Labs. (2024). In Moleculera Labs. https://www.moleculeralabs.com/what-does-the-cunningham-panel-measure