



Should I lower saturated fat in my diet to lower my cholesterol?
Yes, No, Maybe is the only accurate answer.

I have been obsessed lately about cholesterol lowering and have been working on revising my clinic guidelines for reviewing lipid panels and providing guidance and advice.
It is not an easy task as there is so much new information in the space of lipidology as well as some old theories that seem to dominate the mindset. Plus, social media influencers , social media doctors, and health information authors have people asking their doctors for new testing such as Lp(a) and Apolipoprotein B.
Patients are becoming increasingly worried and increasingly confused.
Not a good combo.
A better goal is to become increasingly more prepared and more clear.
Currently, there are two competing views of heart disease between the “Lipid Hypothesis” and “Vascular Inflammation Theory of Heart Disease” . And each of them doesn’t seem to hold its wait in isolation and we need to learn from both of them to have the most comprehensive approach to preventing and treating cardiovascular disease.
When you get back your cholesterol panel ;there are generally three numbers that the health care provider will zero in on. One is Triglycerides (TG). Two; is Low Density Lipoprotein (LDL). These are generally called “bad cholesterol”. Then there is a third number called High Density Lipoprotein (HDLP sometimes called “good” cholesterol
These good vs. bad terms are not really accurate because there can be dysfunctional HDL (sometimes seen when HDL is excessively high) and there can also be low harm LDL (based on the buoyancy of the LDL).
Yet, year after year we are still having the same discussion with our providers.
“ Hey Jack your LDL is high, you need to cut back on Saturated Fat in the diet”
This year Jack pushes back a bit and says to his provider.
“ Doc, with all due respect, you said the same thing last year and I went on a low fat diet all last year, and ate boat loads of fiber and the LDL didn’t budge. Do I need to cut back on Saturated Fat to Lower my LDL?”
Let me repeat that.
“Do I need to cut back on Saturated fat to lower LDL?”
Let’s be clear this is different than saying to I need to cut back on the foods that contain Saturated Fat .

Completely different question.
Foods that are high in saturated fat may cause other problems based on how they are prepared . For example grilled or charred meats may cause advanced glycation end products which may increase other risk factors for heart disease like insulin resistance. And the same can be said for ultra processed foods (UPF)…hello donuts!
But to answer the question with accuracy on the importance of Low Saturated Fat diet; the provider must dig a bit deeper.
The first thing to answer the question is to look at the patients Triglycerides.
Triglycerides (TG) tell a lot about perhaps the inflammation level in the diet that may be in part be attributed to insulin resistance. Insulin increases HMG-CoA reductase, hepatic lipase (HL) activity, and cholesteryl ester transfer protein (CETP). This leads to increased triglyceride production, as well as the formation of small, dense LDL particle. So knowing TG levels tells a lot about how to answer this question.
The second is to consider if the patient may be a hyper-absorbers.
Dr. Thomas Dayspring who is a “ Dr.’s Dr.” and considered a worldwide expert on lipids states that 20%, or so, of people who are cholesterol hyper absorbers. Meaning that in certain people saturated fat intake would increase LDL.
Absorption of Cholesterol depends on Niemann-Pick C1-like 1 (NPC1L1) is a protein that acts as a cholesterol influx receptor, facilitating the absorption of cholesterol from the gut lumen into the enterocyte cell . Some people genetically have a lot of this protein which can increase the absorption. (see image below)
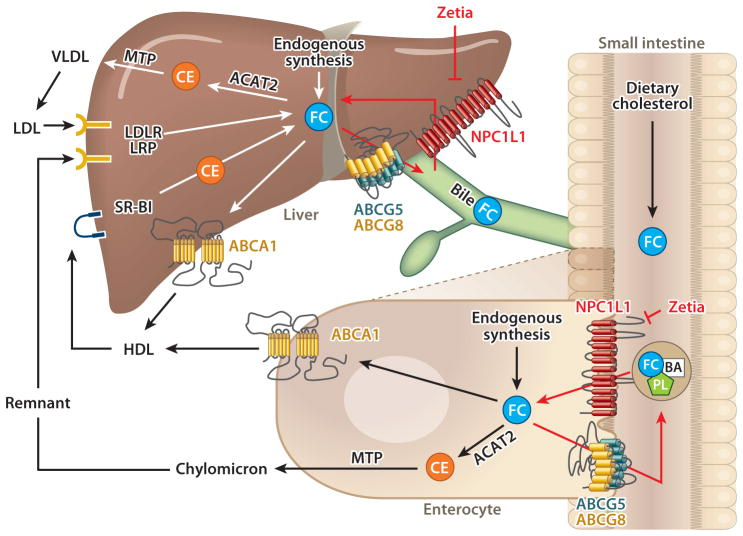
Other genetic factors can influence absorption including transporters ABCG5 and ABCG8. (See image above),
According to Dr. Dayspring; these transporters work together in the intestine and liver to limit cholesterol absorption and to remove excess cholesterol from the body. In the intestine, ABCG5/G8 prevents cholesterol and phytosterols (plant cholesterol) from being absorbed into the bloodstream, by pumping cholesterol and phytosterols back into the intestinal lumen to be excreted.
In liver, ABCG5/G8 is a backup system, controlling cholesterol and phytosterols if they somehow pass through the intestine. The liver then expresses these proteins to send the excess cholesterol through the bile and back to the intestine to be excreted.
Some people have a partial loss of function of the ABCG5/G8 proteins, which can result in hyperabsorption of cholesterol. Most people with this issue are put on Fibrates like Zetia as the picture above depicts.
The Boston Heart Lab has a panel that measures the balance between cholesterol absorption and cholesterol production.
It measures markers of increased cholesterol absorption
Beta-Sitosterol and Campesterol ; these markers of absorption are associated with hyperabsorption related genetic disorders. Elevated levels are associated with increased cholesterol absorption and have been shown to be an independent risk factor for CVD in population studies ·
Very high levels are associated with phytosterolemia, a disorder caused by defects in the ATP binding cassette transporters ABCG5 and ABCG8 . In this disorder, phytosterols in the intestinal cell are retained and there is increased absorption of phytosterols and cholesterol. Most people who have this disorder will need to take a Fibrate like Ezetimibe for life.Cholestanol; this marker is related to increase conversion of cholesterol to a a bile acid chenodeoxycholic acid; which is associated with lipid-disorder-related Xanthomas.

Xanthomas

The test also measures markers of increased cholesterol production by the body including
Lathosterol; which when elevated means increased LDL-production secondary to insulin resistance, obesity and familial combined hyperlipidemia.
Desmosterol; which elevated levels are associated with increased cholesterol production or decreased conversion of desmosterol to cholesterol · Moderate elevations have been associated with a significant increased risk of cognitive decline with aging.
So lets update the conversation in 2024 between Jack and his provider
Do I need to cut back on Saturated fat to lower LDL?
Today the Dr. states the following
“Jack , your Triglycerides are very good and you don’t have any signs of insulin resistance. Also your HDL is in a healthy range.. You state you are not eating a lot of fried or grilled animal products. This year I would not state a low saturated fat diet is needed. As always eat predominantly unsaturated or monounsaturated fats due to their positive effect on inflammation; but I see no reason for you to go on a low saturated diet”
Jack pushes back. “So what should I do, what should I eat, I am confused!”
The Dr. responses
“ LDL does matter as does the burden it has had on your arteries over the years. Your Diet may be perfectly healthy as it can be but your body may producing higher amounts of LDL independent of your diet. Let’s consider doing an NMR- lipoprofile, Lipoprotein little (a), Apoprotein B (APOB), LpA2, Homocysteine, ADMA, and CT calcium score and see if we can detect reasons to to take supplements, medications, or alter other factors in your diet and lifestyle to lower ldl”
Note: this reasoning will be covered in another upcoming post.
Now to the patient that lowered saturated fat in the diet , and there LDL went down in the serum.
For this patient they may indeed look at the absorption panel to confirm hyper absorbers status.
Because staying on a low saturated diet long term is difficult and even in some cases a plant based diet would not even lower the LDL enough to prevent heart disease on any accumulative level.
So these patient may need specific medications like Fibrates in combinations with HMG-COA-reductase inhibitors to block absorption and reduce production.
In summary:
The Lipid panel (basic) is obviously not enough when the levels come back repeatedly normal. Yet, it is fine for global/public screening but as an individual it doesn’t answer enough questions.
A fusion of the classic lipid hypothesis with all the rich information and understanding of the vascular inflammation approach is truly needed to wrap our head around lipid disorders and CV disease.
Lowering Saturated Fat in the diet may have no influence on your LDL levels as one may be an excess producer of LDL for genetic reasons. Yet saturated fat in other food forms that are proinflammatory may actually lead to increased LDL production.
Knowing and modifying why someone is an excess producer of LDL is a key question to answer
Knowing if someone is hyper-absorber is especially important for some who appear to have some saturated-fat intake influence on their LDL levels.
One final comment; knowing all this information is great. But in rare circumstances we still get caught off guard where a patient has lifelong perfect Lipid Panels, normal Glucose, Normal Blood pressure and then we find out they have signifcant heart disease. This happened in my Father’s case , albeit, he was a smoker for 25 years.
So we can never be so sure and if you have a family history of cardiovascular disease especially pre-70 years old; you should visit a cardiologist or provider that will do a deep dive of imaging, echocardiogram, and deep lipid testing. Don’t be fooled by basic blood tests.
I welcome your comments and reactions below as I am on a lifelong journey of learning and continuous improvement.
And on a personal note; on a mission to have the healthiest heart and brain I can for many many years to come.
====================
You can keep up with my ever evolving lipid modification protocol here
Related posts
Arachidonic Acid to EPA ratio

It’s the one year anniversary of my Father’s death (he’s #32 in this picture from Brooklyn Tech); and I have done a lot of reflection and shed some tears .
Vascular Health and the Glycocalyx with Dr. Kristine Burke

Episode 95: Cardiovascular endothelial health with Dr. Kristine Burke. Is now live.
David Feldman is a curious amateur medical researcher who has proposed the "lean mass hyper-responder" hypothesis that says some people respond very differently to dietary fat. I'm curious to know if you have comments about his conclusions, such as this evidence that for some people a diet of Oreos can actually *lower* LDL levels, demonstrating that obviously LDL lowering is not the be all and end all:
https://pmc.ncbi.nlm.nih.gov/articles/PMC10818743/